
Research Article | DOI: https://doi.org/10.31579/2578-8868/012
1 Department Social Neuroscience, Zimbabwe.
*Corresponding Author: Melina Oison,Department Social Neuroscience, Zimbabwe
Citation: Melina Oison, Juniper Drakken,Deep Brain Stimulation in Treatment of Mental Illness,Doi: 10.31579/2578-8868/012
Copyright: © 2017 Melina Oison. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 January 2017 | Accepted: 28 January 2017 | Published: 11 February 2017
Keywords: hydromolecular hypothesis; dehydration; dementia
Abnormalities of water homeostasis can be early expressions of neuronal dysfunction, brain atrophy, chronic cerebrovasculopathy and neurodegenerative disease. The aim of this study was to analyze the serum osmolality of subjects with cognitive impairment.The hydromolecular hypothesis intends to explain the relationship between dehydration and cognitive impairment in older patients as the result of protein misfolding and aggregation, in the presence of a low interstitial fluid volume, which is a defect of the microcirculation. Defective proteins were shown to impair the amount of information in brain biomolecular mechanisms, with consequent neuronal and synaptic damage.
The regulation of water balance is governed by a feedback mechanism involving the function and interaction of different regions of the central nervous system and the kidneys. Plasma osmolality indicates the level of body hydration and hypothalamus osmoreceptors detect and are sensitive to its variations. High plasma osmolality, increased to levels above a physiologic threshold (290 to 295 mOsm per kilogram of water), leads to secretion of the peptide hormone, vasopressin, from the vasopressinergic nerve endings in the neurohypophysis. Vasopressin binds receptors in the kidney that decrease the excretion of water, and subsequently, a greater fraction of filtered water is returned to the blood. This process lowers the plasma osmolality, reduces the stimulus for vasopressin secretion and thirst and completes the feedback loop. Failure of this mechanism, which is commonly observed in hospitalized patients, results in a variety of water balance disorders. More recent evidence has clarified that the aging process is commonly related to multiple abnormalities in water homeostasis, highlighting its effects on morbidity, cognition, osteoporosis, fractures, gait instability, and mortality. In older patients, water homeostasis regulation can be altered because of multifactorial mechanisms, such as renal function alterations, body composition and hypothalamic–pituitary regulation of thirst and vasopressin secretion changes.
The present study was conducted according to the Declaration of Helsinki, the Guidelines for Good Clinical Practice and the Guidelines for Strengthening the Reporting of Observational Studies in Epidemiology, and it was approved by the local ethics committee for human experimentation (Prot. No. 3877/DS). The study was an observational study, in which the assignment of an intervention to the participants, its effect assessment and health-related biomedical or behavioural outcomes are not considered. In the present study, healthy participants were recruited as control subjects.
Inclusion criteria were as follows: (1) age ≥65 years; (2) diagnosis of a subjective cognitive impairment (SCI) according to the Subjective Cognitive Decline Initiative (SCD-I) Working Group ; (3) diagnosis of late-life depression (LLD) according to the (Diagnostic and Statistical Manual of Mental Disorders Fifth Edition) DSM 5 criteria; (4) diagnosis of mild cognitive impairment (MCI) according to the National Institute on Aging—Alzheimer’s Association (NIAAA) criteria; (5) diagnosis of Alzheimer’s disease (AD) according to the NIAAA criteria; (6) diagnosis of Lewy body disease (LBD) according to the (Dementia with Lewy bodies) DLB consortium criteria; (7) diagnosis of vascular dementia (VaD) according to the criteria of the National Institute of Neurological Disorders and Stroke—Association Internationale pour la Recherche et l’Enseignement en Neurosciences (NINDS-AIREN) [work group; (8) the ability to provide informed consent or the availability of a relative or legal guardian in the case of severe demented patients. The exclusion criteria were as follows: (1) diagnosis of mixed dementia (MxD); (2) presence of a serious comorbidity, tumors, other diseases or physiological status (ascertained blood infections, vitamin B12 deficiency, anemia, disorders of the thyroid, kidneys, or liver), that could be causally related to cognitive impairment; (3) history of alcohol or drug abuse, head trauma, and other causes that could cause memory impairment.
For dichotomous variables, hypotheses regarding differences between groups were tested using the Fisher’s exact test. This analysis was made using the 2-Way Contingency Table Analysis.
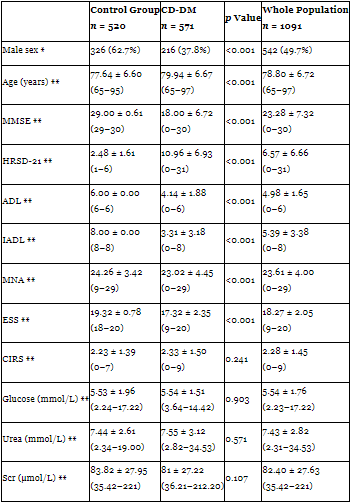
During the enrolment period, 1135 older patients were screened for inclusion in the study. Of these, nine patients were excluded because they were younger than 65 years, 12 patients had an incomplete examination and 23 patients had MxD. Thus, the final population included 1091 patients, 542 men (49.70%) and 549 women (50.3%), with a mean age of 78.80 ± 6.72 years and an age range from 65 to 97 years. Therefore, 520 patients (Male: 326, Female: 194; mean age of 77.64 ± 6.60 years, range 65–95 years) were included in the control group, and 571 patients (Male: 216, Female: 355; mean age of 79.94 ± 6.67 years, range 65–97 years) had cognitive decline and/or depression mood (CD-DM). The demographic and clinical characteristics of the control group and patients with CD-DM are summarized in Table 1.
Demographic and clinical characteristics of control group and patients with cognitive decline and/or depression mood (CD-DM).
Dehydration has been reported to be the most common fluid and electrolyte imbalance in older adults [. Recent clinical studies have shown that the hydration state affects cognitive performance, particularly visual attention and mood.The changes in extracellular osmolality inevitably affect the intracellular environment determining important alterations in the volume and function of cellular mechanisms causing irreversible morphological and functional damage. Thus, these changes could be major contributing factors to age-related neurovascular vulnerabilities and are currently under intense investigation as potential therapeutic targets. It has been hypothesized that chronic hypovolemia, due to hypohydration, is perhaps one of the principal mechanisms behind the development of obesity, diabetes, hypertension, and even Alzheimer’s disease. Hospitalized older adults suffering from dehydration have been reported to have mortality rates as high as 45–46%, but only a few studies exist regarding water intake and excretion in older patients.
Conclusion
Thus, dehydration among patients with Alzheimer's disease is an issue that nursing staff must recognize. Nursing staff should receive the appropriate education in order to address the issue of dehydration with this population. Having a plan of care for hydration for each patient may identify the barriers of hydration and lead to interventions that are needed to decrease the risk of dehydration. Interventions to overcome these hydration barriers must be developed, implemented, and evaluated not only by the nursing staff but by the family members. This collaborative effort may decrease the chances of a patient from becoming dehydrated and having to be treated for dehydration.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
